In Denmark, approximately 25% of all births are induced. There are many different reasons for inducing birth. The common reason for induction of labour is that the condition of the mother or the fetus indicates that the pregnancy should be completed within a few days.
 Examination before induction of labour
Examination before induction of labour
When you meet at the ward to start induction of labour, the midwife starts by
making sure that both you and your fetus are well.
This is done by initiating a so-called CTG where the fetal heart rate and the
contractions of the uterus are monitored for at least 20 minutes.
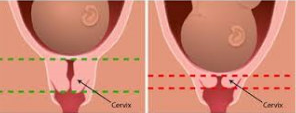
A vaginal examination will be performed by the midwife to assess cervical length, dilation, and the position of the head in your pelvis. Based on an overall
assessment, we plan the further course in collaboration with you.
When the time of birth draws closer, the cervix ”matures”, which means it gets softer. The cervix starts to open a little.
Induction of labour can be done in several ways:
- Maturation of the cervix with the hormone Misoprostol.
- Rupture of membranes - i.e. the amniotic sac is ruptured and the
water breaks. - Starting intravenous administration of medicine to stimulate contractions.
- Insertion of a balloon catheter.
 Labour induction procedure
Labour induction procedure
There are several reasons for choosing to place a balloon catheter.
- If you have previously had a Caesarean section, labour cannot be induced by Misoprostol.
- If the midwife is unsuccessful rupturing the membranes despite treatment with Misoprostol for several days.
- If you do not wish to be treated with Misoprostol.
The balloon is a thin flexible catheter inserted through the cervix and then filled with water; the balloon expands and puts pressure on the cervix. This treatment is normally not painful.

 Kontakt
Kontakt
How to contact us
Maternity Ward
Strandpromenaden 35D
8700 Horsens
Change of appointment
The Maternity Wards secretary: All weekdays at 10.00 am - 12.00 am at phone 7842 6460
Non-immediate questions
The midwife counselling: All weekdays at 8.00 am - 9.30 am at phone 7842 6470
Immediate questions and delivery
Maternity Ward: 78 42 99 03
Before 20th week of pregnancy: general practitioner or duty doctor.
If you follow the known midwife solution you must call the hotline telephone number you have been provided by your consulting midwife.
Gå direkte til:
Brug ikke informationen på denne side til at stille dine egne diagnoser, og følg kun instruktionerne i vejledningen, hvis hospitalet har henvist dig til siden.